Your Acid Reflux Medication Is Starving Your Cells: The Hidden Cost of PPIs
Proton pump inhibitors nutrient deficiency is a hidden crisis. Learn how PPIs disrupt mineral absorption, redistribute nutrients, and what to do instead.
Medical Disclaimer
This content is for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
If you have ever been handed a prescription for omeprazole, lansoprazole, or another proton pump inhibitor and told to "just take it," you are not alone. Over 15 million Americans use PPIs regularly, and many stay on them for years, sometimes decades, without a second thought. These medications rank among the most prescribed drugs on the planet. But here is what your doctor likely never mentioned: proton pump inhibitors nutrient deficiency is a well-documented, progressive problem that quietly undermines your health from the inside out. Every time you suppress stomach acid, you are not just silencing a symptom. You are disrupting one of the most fundamental processes your body relies on to extract energy from food. And the consequences reach far beyond your digestive tract, affecting your bones, your brain, your blood, and the mitochondria that power every cell in your body.
This is not about scaring you off your medication. It is about giving you the information you need to make an empowered decision. Over the next several minutes, you will learn exactly how PPIs interfere with nutrient absorption, why your standard lab work may be hiding the damage, what the research actually shows about long-term consequences, and most importantly, what you can do about it. At Biospark Health, we believe that understanding root causes is the first step toward real recovery, and when it comes to acid reflux, the root cause is almost certainly not what you have been told.
The Hidden Nutrient Crisis Inside Every PPI Pill
To understand why proton pump inhibitors nutrient deficiency is so widespread, you need to understand what stomach acid actually does. Hydrochloric acid is not some unfortunate byproduct of digestion. It is the master key that unlocks nutrients from food. Without adequate acid, your body cannot properly liberate minerals from food matrices, activate pepsin (the enzyme responsible for breaking down protein), convert certain vitamins into their absorbable forms, or maintain the low pH required for ionizing key minerals like calcium, magnesium, iron, and zinc.
PPIs work by permanently disabling the proton pumps in your stomach lining. These are the tiny molecular machines that produce hydrochloric acid. When you take omeprazole or a similar PPI, you are shutting down up to 70% of your acid-producing capacity. The intended effect is less acid, less burning. The unintended effect is a slow, systemic starvation of the nutrients your cells depend on for energy production.
It Is Not Just Depletion. It Is Redistribution.
Here is where the story gets more nuanced than most doctors realize. A study published in ACS Omega tracked mineral levels in subjects given omeprazole over 10, 30, and 60 days. The researchers did not simply measure whether mineral levels dropped. They measured where those minerals went. What they found was striking. Minerals like calcium, magnesium, zinc, and iron did not just vanish from the body. They redistributed. Blood levels shifted. Concentrations in the stomach lining, liver, and spleen changed in unexpected patterns. Some minerals accumulated in certain tissues while becoming depleted in others.
Think of it like a supply chain disruption. When a major shipping port shuts down, goods do not simply disappear. They pile up in the wrong warehouses, get rerouted to the wrong destinations, and leave critical locations empty. That is what happens inside your body when PPI nutrient absorption is compromised. The minerals are still present, but they are in the wrong places, in the wrong concentrations, unavailable to the cells that need them most.
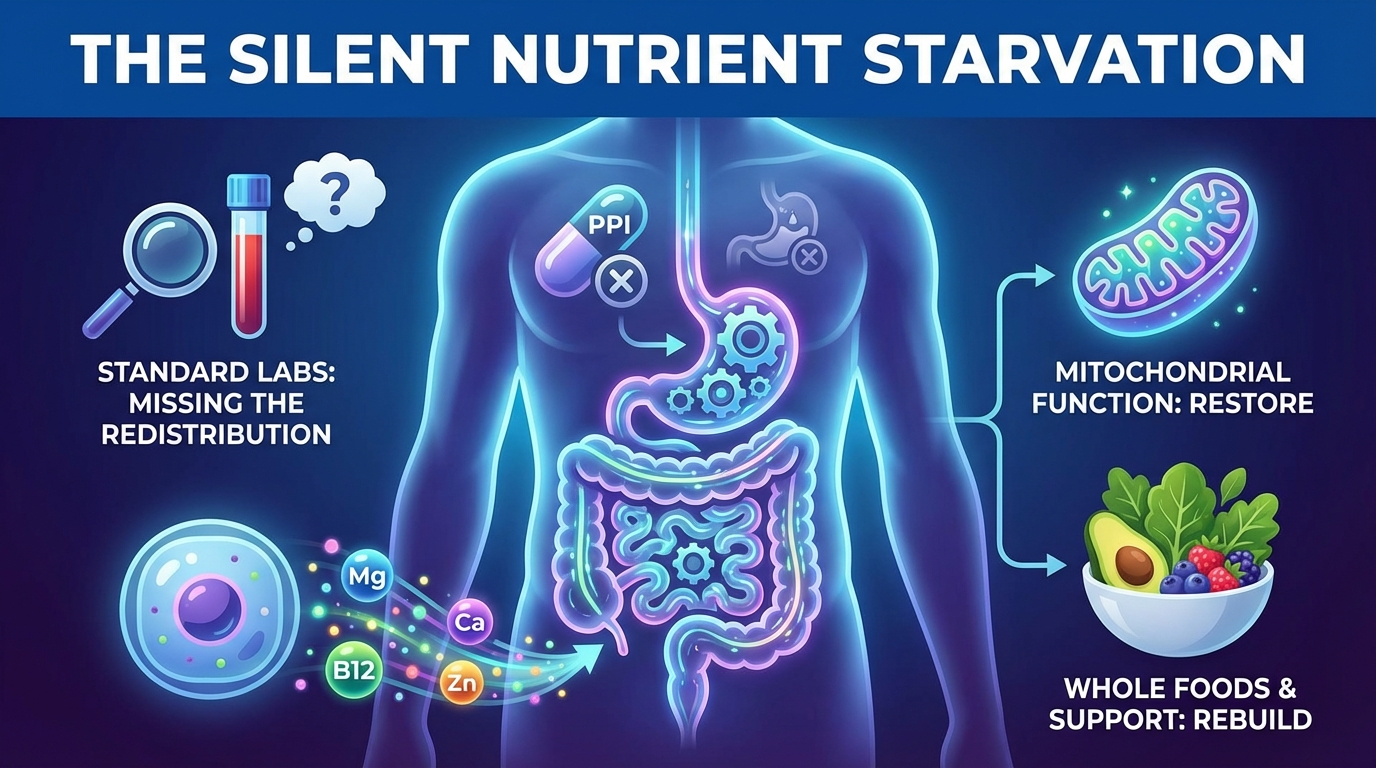
This redistribution pattern explains something that frustrates both patients and practitioners: why someone can be on a PPI for years, feel progressively worse, and still have lab work that looks "within range." The standard serum test is checking one warehouse (your blood) while the real shortage is happening in your bones, your brain, your mitochondria.
Why "Just Take Supplements" Falls Short
The reflexive advice many patients receive is to simply take a multivitamin or add a calcium supplement. But this fundamentally misunderstands the problem. If your stomach cannot produce enough acid to break down and absorb nutrients from food, it cannot efficiently absorb nutrients from supplements either. You are pouring water into a bucket with a hole in it. Some supplementation strategies can help (and we will discuss those later), but they must be paired with addressing the underlying cause of low stomach acid nutrient absorption. Anything less is just symptom management layered on top of more symptom management.
Why Your Lab Results Look Normal While Your Body Is Starving
One of the most dangerous aspects of omeprazole vitamin deficiency is how long it hides in plain sight. Patients take their PPI faithfully, get annual bloodwork, see values in the "normal" range, and assume everything is fine. Meanwhile, their energy declines. Their thinking gets foggy. Their bones thin. Their immune system falters. And nobody connects the dots.
The B12 Evidence Is Damning
A systematic review published in Cureus analyzed data from 693 participants across multiple studies examining the relationship between PPI use and vitamin B12 status. The findings were consistent and concerning. Participants using PPIs for 12 months or longer showed B12 level drops of 12 to 18 percent compared to controls. This may sound modest, but B12 operates on a razor-thin margin. Even subclinical deficiency (levels that still technically fall within the "normal" lab range) can produce fatigue and weakness, memory problems and cognitive decline, peripheral neuropathy (tingling and numbness), mood disturbances including depression and anxiety, and impaired methylation, a process critical for DNA repair and detoxification.
The connection between omeprazole vitamin B12 deficiency and cognitive decline is particularly alarming. B12 is essential for maintaining the myelin sheath that insulates your nerves. When B12 drops, nerve conduction slows. Thinking becomes harder. Reaction times increase. In older adults, this can be misdiagnosed as early dementia or simply attributed to "normal aging." But there is nothing normal about nutrient starvation caused by a medication.
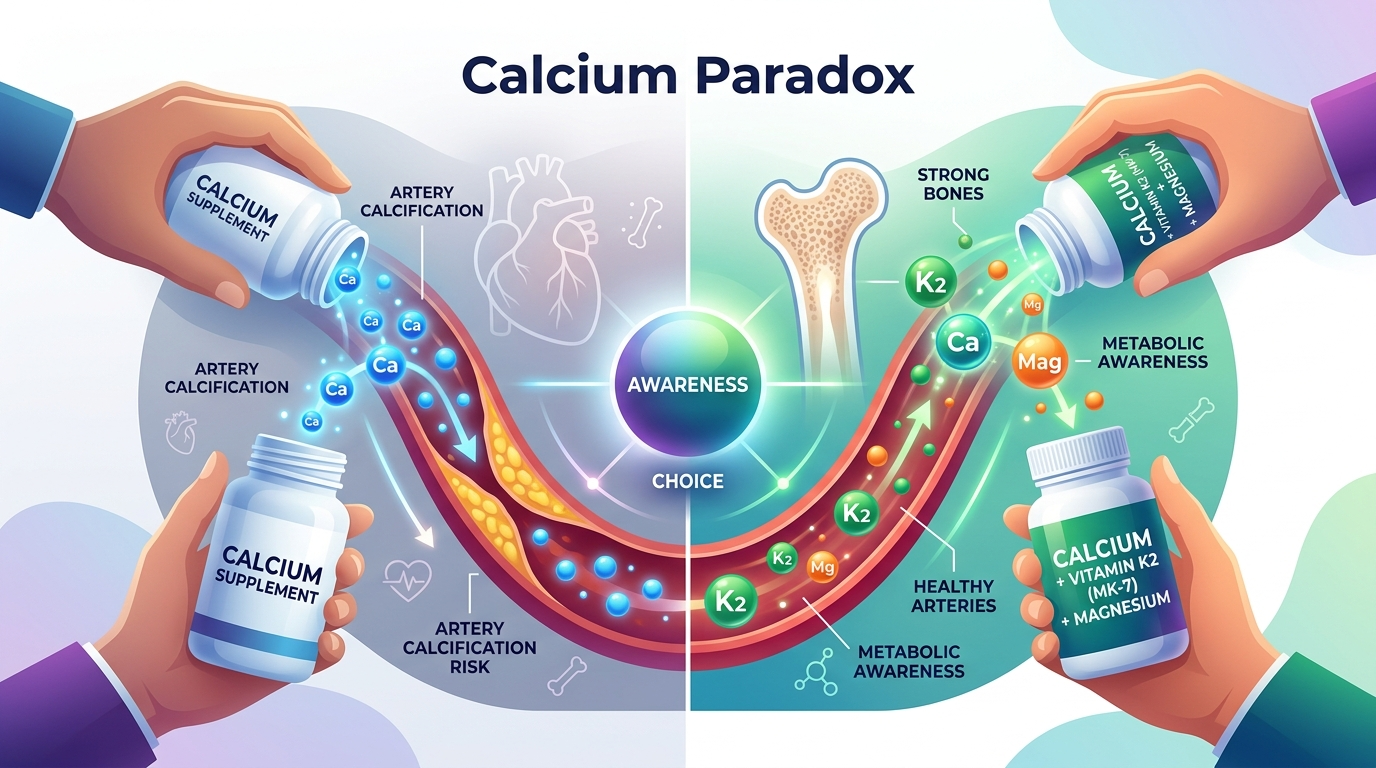
Calcium, Bones, and Falls
The systematic review also documented shifts in calcium metabolism among long-term PPI users. Calcium requires an acidic environment for proper absorption. When you suppress acid chronically, calcium absorption drops, and your body begins pulling calcium from your bones to maintain blood levels. This is why long-term PPI use has been associated with increased fracture risk, particularly hip fractures in older adults. The FDA has issued warnings about this since 2010, yet millions of people remain on these medications without bone density monitoring or calcium absorption support.
The downstream consequences compound: weakened bones lead to fractures, fractures lead to immobility, immobility leads to further metabolic decline. For older adults, a hip fracture can be a life-altering event, and proton pump inhibitors nutrient deficiency may be a significant, preventable contributing factor.
Polypharmacy Makes Everything Worse
Many PPI users are not taking just one medication. They are on multiple drugs, each with its own nutrient-depleting effects. Metformin reduces B12. Diuretics deplete magnesium and potassium. Statins interfere with CoQ10 production. Layer a PPI on top of that cocktail, and you have created a perfect storm of nutrient depletion that no single lab test is designed to catch.
Standard bloodwork measures serum levels, which represent what is circulating in your blood at a single moment in time. It does not measure intracellular levels (what is actually inside your cells), tissue-specific concentrations (what is available in your bones, brain, or organs), or functional status (whether your enzymes and mitochondria have enough of these nutrients to do their jobs). This is why someone can have "normal" magnesium on a blood test while their cells are running on empty. The blood is the last place the body allows levels to drop, because it prioritizes keeping blood chemistry stable, even at the expense of every other tissue.
When Acid Suppression Becomes a Medical Emergency
If the gradual erosion of nutrients sounds concerning, consider what happens when chronic acid suppression collides with other risk factors. The consequences can be severe and even life-threatening.
A Case Study in Scurvy: Yes, Scurvy
A case report published in BMJ documented a man in his 50s who developed scurvy, the same disease that plagued 18th-century sailors. His vitamin C levels had dropped to critically low levels, producing symptoms that included fatigue and weakness, bruising and poor wound healing, swollen and bleeding gums, joint pain and muscle aches, and psychological changes including depression. The cause was a combination of long-term PPI use (which suppressed his ability to absorb vitamin C from food) and a diet that was already limited in fresh produce. Neither factor alone would likely have produced scurvy. But together, they created a catastrophic nutritional failure.
This case illustrates a principle that Dr. Presciutti emphasizes with patients at Biospark Health: chronic medication use does not exist in a vacuum. It interacts with your diet, your lifestyle, your stress levels, and your overall metabolic function. When multiple factors converge, the body's reserves can be overwhelmed far faster than anyone expects.
The Compounding Effect
PPI nutrient absorption problems rarely produce a single, dramatic symptom. Instead, they create a slow cascade. Reduced acid leads to reduced nutrient extraction. Reduced nutrients lead to reduced cellular energy production. Reduced cellular energy leads to reduced digestive function. Reduced digestive function leads to even less acid production. Each turn of the cycle makes the next turn worse. And because the decline is gradual, most people adapt to feeling progressively worse without ever identifying the cause.
The Root Cause Most Doctors Get Backwards
Here is the part that challenges the standard medical narrative, and it is the single most important thing you will read in this article. Most acid reflux is not caused by too much stomach acid. It is caused by too little.
The Valve That Runs on Acid
At the top of your stomach sits a muscular valve called the lower esophageal sphincter (LES). This valve is supposed to close tightly after you swallow, preventing stomach contents from splashing back up into your esophagus. But here is what most people, including many doctors, do not realize: the LES requires adequate stomach acid to signal it to close properly.
When stomach acid levels are sufficient, the low pH triggers the LES to tighten. When acid levels drop (whether from aging, stress, nutrient deficiency, or chronic PPI use), the LES loses its signaling cue and relaxes. Even a small amount of acid in a low-acid stomach can then splash upward, causing the burning sensation we call reflux.
So what happens when you treat this with a PPI? You lower acid even further. The LES gets even less signaling. The valve stays even more relaxed. The reflux may temporarily improve because there is less acid to burn, but the underlying mechanical dysfunction gets worse. You have not fixed the problem. You have suppressed the symptom while deepening the cause.
The Vicious Cycle
This creates what functional practitioners recognize as a self-reinforcing decline. Low stomach acid impairs nutrient absorption. Poor nutrient status reduces the body's ability to produce stomach acid (acid production is an energy-intensive process that requires zinc, B vitamins, chloride, and robust mitochondrial function). Less acid means less nutrient absorption. Less nutrient absorption means even less acid. Round and round it goes, with each cycle leaving the patient more depleted and more dependent on the medication.
This is not speculation. It is basic physiology. The parietal cells that produce hydrochloric acid are among the most mitochondria-dense cells in the entire body. They require enormous amounts of cellular energy to pump hydrogen ions against a concentration gradient. When mitochondrial function is compromised by nutrient deficiency, these cells simply cannot do their job. The result is a progressive decline in acid production that PPIs accelerate, not resolve.
Pepcid as a Safer Bridge
For patients who need symptom relief while addressing root causes, famotidine (sold as Pepcid) represents a more measured approach than PPIs. Unlike proton pump inhibitors, which permanently disable acid-producing pumps, famotidine is an H2 blocker that temporarily reduces acid production and wears off within hours. This allows acid production to resume between doses, preserving some digestive function.
Famotidine also has an interesting secondary property that is gaining attention in functional medicine circles: it influences serotonin signaling. Given that the gut produces roughly 90% of the body's serotonin, this interaction may have implications for mood, motility, and the gut-brain axis that extend beyond simple acid suppression. While famotidine is not a long-term solution either, it can serve as a useful transitional tool while someone works on restoring proper digestive function. Supplements to take with PPI medications during a tapering phase should be selected carefully and ideally guided by a practitioner who understands the full picture.
The Biospark Approach: Restoring Digestive Function at the Cellular Level
At Biospark Health, Dr. Presciutti takes a fundamentally different approach to acid reflux and digestive dysfunction. Rather than asking "how do we suppress the symptom," the question becomes "why is the body producing this symptom, and what does it need to heal?"
Start with the Mitochondria
Since acid production depends on robust cellular energy, recovery begins with supporting mitochondrial function. This means removing obstacles to energy production (including seed oils, which impair mitochondrial membrane function and promote inflammation) and providing the raw materials cells need to generate ATP efficiently. A metabolism-first approach recognizes that digestive function is not separate from overall metabolic health. It is a direct expression of it.
Taper Thoughtfully
Abruptly stopping a PPI after long-term use can trigger rebound acid hypersecretion, a temporary but intense surge in acid production that can make reflux dramatically worse. This is why so many patients feel unable to quit. The key is a slow, methodical taper, ideally supervised by a knowledgeable practitioner. Reducing the dose gradually over weeks or months, while simultaneously building up digestive capacity, allows the body to recalibrate without crisis.
Rebuild with Whole Foods and Targeted Support
Recovery from proton pump inhibitors nutrient deficiency requires more than just popping a multivitamin. It requires a dietary foundation built on nutrient-dense whole foods that are easy to digest and absorb. Well-cooked root vegetables, ripe fruits, bone broth, high-quality dairy (for those who tolerate it), and properly prepared proteins provide the building blocks cells need.
Targeted support may include digestive bitters taken before meals to stimulate natural acid production, betaine HCl with pepsin to temporarily supplement acid levels during recovery, and specific nutrients like B12 (in methylcobalamin form), magnesium, zinc, and fat-soluble vitamins. But these supplements to take with PPI medications or during tapering should be part of a comprehensive strategy, not a band-aid applied in isolation.
Address the Whole System
Dr. Presciutti's bioenergetic approach recognizes that digestive dysfunction is rarely an isolated problem. It connects to thyroid function, stress hormone balance, liver health, and overall metabolic rate. When you restore cellular energy production across the whole system, digestive function often improves as a natural consequence. The body knows how to make stomach acid. It just needs the energy and raw materials to do so.
Ready to restore your metabolism at the cellular level?
The Bioenergetic Reset Program addresses root causes, not symptoms. Join 300+ members who've discovered what real metabolic health feels like.
- 9+ hours of comprehensive training
- Twice-monthly LIVE coaching calls
- Complete meal plans & protocols
- Direct email support
/month | Cancel anytime
Digestive Health Support in Reading and Berks County, PA
If you live in southeastern Pennsylvania and have been struggling with chronic acid reflux, digestive discomfort, or concerns about long-term PPI use, Biospark Health is here to help. Located in the Reading and Wyomissing area, Dr. Presciutti works with patients throughout Berks County and the surrounding communities to address digestive health at its root.
Unlike conventional approaches that focus on suppressing symptoms indefinitely, Biospark Health's metabolic and bioenergetic framework is designed to help your body restore its own digestive capacity. Whether you are looking for an acid reflux specialist in Berks County, need guidance tapering off a PPI safely, or simply want to understand why you have been feeling progressively worse despite "normal" lab results, this practice offers a different path forward.
Biospark Health proudly serves patients from Reading, Wyomissing, Lancaster, Downingtown, Allentown, West Chester, and the broader southeastern Pennsylvania region. Both in-person and virtual consultations are available, making expert digestive health support in Reading, PA accessible no matter where you are in your health journey.
Frequently Asked Questions
Which nutrients are affected by proton pump inhibitors?
Proton pump inhibitors nutrient deficiency can affect a wide range of essential nutrients. The most well-documented include vitamin B12, calcium, magnesium, iron, zinc, and vitamin C. However, because stomach acid is required for the proper breakdown and absorption of most minerals and many vitamins, the true scope of nutrient impact is likely broader than clinical research has fully captured. Fat-soluble vitamins (A, D, E, K) may also be affected, since fat digestion requires adequate acid and enzyme activity. The key insight is that this is not a simple "one nutrient" problem. It is a systemic disruption of the body's ability to extract nutrition from food.
Can omeprazole cause nutrient deficiency?
Yes. Research consistently demonstrates that omeprazole vitamin deficiency is a real and measurable consequence of long-term use. The Cureus systematic review of 693 participants showed B12 declines of 12 to 18 percent after 12 months. The ACS Omega study demonstrated mineral redistribution across multiple organ systems. The FDA has issued warnings about magnesium depletion and fracture risk. While short-term use (two to four weeks) for acute issues carries less risk, the problem is that most PPI prescriptions are renewed indefinitely, turning a short-term intervention into a long-term metabolic burden.
Should I take a magnesium supplement if I take a PPI?
Magnesium supplementation may be beneficial for PPI users, but it is not a complete solution. Low stomach acid nutrient absorption means that many oral magnesium supplements will not be absorbed efficiently either. Forms like magnesium glycinate or magnesium bicarbonate tend to be better absorbed than magnesium oxide. Topical magnesium (such as magnesium chloride applied to the skin) can bypass the digestive system entirely. However, the most important step is working toward restoring proper acid production so that your body can absorb magnesium from food the way it was designed to.
What do you crave when your B12 is low?
B12 deficiency can manifest as unusual cravings, particularly for ice (a condition called pagophagia, which is more commonly associated with iron deficiency but can overlap), red meat, and other protein-rich foods. Some people report cravings for sour or acidic foods, which may represent the body's attempt to stimulate acid production. However, cravings are an unreliable indicator of deficiency. Many people with omeprazole vitamin B12 deficiency experience fatigue, brain fog, numbness or tingling in extremities, mood changes, and difficulty concentrating long before specific cravings develop. If you have been on a PPI for more than a few months, testing your B12 level (ideally through a methylmalonic acid test, which is more sensitive than serum B12) is far more reliable than waiting for cravings.
How can digestive health be restored after long-term PPI use?
Restoring digestive function after prolonged PPI use requires a multi-step approach. First, work with a knowledgeable practitioner to taper your PPI slowly, reducing the dose over weeks or months to avoid rebound acid hypersecretion. Second, support acid production with digestive bitters, apple cider vinegar before meals, and (when appropriate) betaine HCl supplementation. Third, focus on a nutrient-dense, whole-food diet that emphasizes easy-to-digest proteins, well-cooked vegetables, ripe fruits, and bone broth. Fourth, address mitochondrial function through eliminating seed oils, supporting thyroid health, and ensuring adequate intake of key cofactors like B vitamins, magnesium, and zinc. Fifth, consider working with a functional or bioenergetic practitioner who understands the full metabolic picture. Supplements to take with PPI medications during this transition should be carefully selected based on your individual needs and testing results.
Reclaiming Your Digestive Health
The reality of proton pump inhibitors nutrient deficiency is not a reason to panic, but it is a compelling reason to ask better questions about your health. If you have been on a PPI for months or years, your body has been operating with compromised nutrient absorption for that entire time. The fatigue, the brain fog, the weakening bones, the declining vitality: these are not inevitable consequences of aging. They may be preventable consequences of a medication that was only ever designed for short-term use.
The good news is that the body has a remarkable capacity for recovery when given the right conditions. Stomach acid production can be restored. Nutrient stores can be rebuilt. Mitochondrial function can be supported. Digestive strength can return. But it requires moving beyond the symptom-suppression model and toward a root-cause approach that respects how the body actually works.
At Biospark Health, this is exactly what we help people do every day. Whether you are just beginning to question your PPI use or you are ready to start a supervised taper, the path forward begins with understanding. Your cells need fuel. Your mitochondria need support. Your stomach needs to do the job it was designed to do.
You deserve more than a prescription that masks the problem. You deserve answers, and a plan that actually moves you toward health.
Learn more about the Biospark approach to metabolic health →
Tags:
References & Citations
This article is supported by scientific research and peer-reviewed sources. Click citations to verify the evidence.
- [1]Gröber U, Schmidt J, Kisters K(2020)Important drug-micronutrient interactions: A selection for clinical practice..Critical Reviews in Food Science and Nutrition.View Source
- [2]Shikh EV, Makhova AA, Chemeris AV, et al.(2021)Iatrogenic deficits of micronutrients..Voprosy pitaniia.View Source
- [3]Dharmarajan TS(2021)The Use and Misuse of Proton Pump Inhibitors: An Opportunity for Deprescribing..Journal of the American Medical Directors Association.View Source
- [4]Choudhury A, Jena A, Jearth V, et al.(2023)Vitamin B12 deficiency and use of proton pump inhibitors: a systematic review and meta-analysis..Expert Review of Gastroenterology & Hepatology.View Source
- [5]Thurber KM, Otto AO, Stricker SL(2023)Proton pump inhibitors: Understanding the associated risks and benefits of long-term use..American Journal of Health-System Pharmacy.View Source
- [6]Freedberg DE, Kim LS, Yang YX(2017)The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association..Gastroenterology.View Source
- [7]Andrawes M, Andrawes W, Das A, et al.(2025)Proton Pump Inhibitors (PPIs)-An Evidence-Based Review of Indications, Efficacy, Harms, and Deprescribing..Medicina.View Source
All references have been reviewed for scientific accuracy and credibility. Citations follow standard academic format and link to original research where available.
About Dr. Steven Presciutti, MD
Founder & Health Coach at Biospark Health, specializing in bioenergetic health and metabolism optimization.